A baby's heart rate was being monitored with a CTG abdominal transducer. The mother's heart rate was also being monitored using a finger probe pulse oximeter, attached to the CTG machine. The mother and baby’s heart rates were displayed visually on the CTG machine and recorded on the CTG trace. It was likely that the abdominal transducer lost contact with the baby’s heart rate and recorded the mother’s heart rate as shown on the CTG trace below.
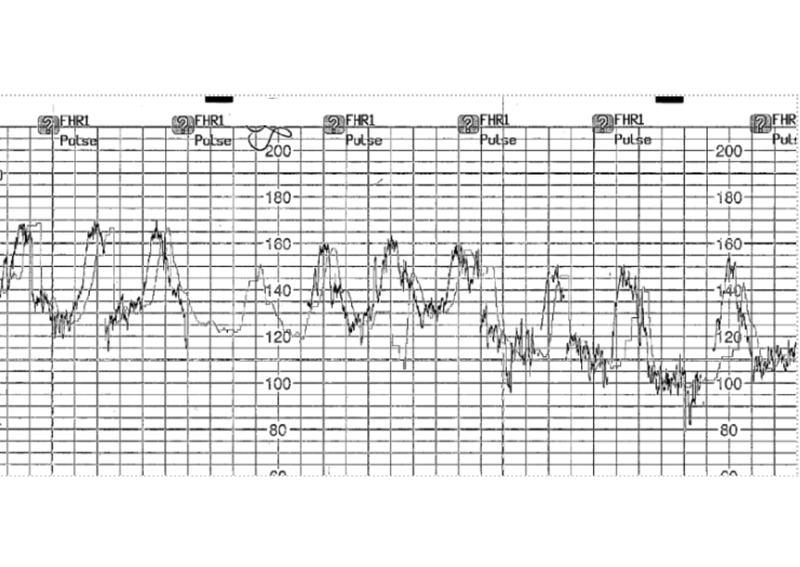
The average calculation time of the maternal pulse from a CTG’s pulse oximeter finger probe can be different to the maternal pulse recorded by an abdominal transducer. This can lead to a delay in the calculation and the recording of the mother’s heart rate, in this example, of up to 12 seconds. This meant that there were two different values being shown on the CTG visual display and this reassured staff that there were two different heart rates being heard, when it was likely to be the mother’s heart rate on both. To prevent a mother’s heart rate being inadvertently interpreted as a baby’s heart rate it is worth considering the following questions:
- Does your training include functionality of the CTG machines used in your Trust including how the machines work and alarm functions?
- Does the manufacturer’s guidance indicate a delay in the calculation and recording of the maternal heart rate for the CTG machines used by your trust?
This was first published in the Stakeholder Bulletin: March 2025 - Edition
Related news
Safety Spotlight: Patient Ethnicity Data Collection
MNSI has found that inaccurate or missing recordings of a woman’s ethnicity have impacted her subsequent pathway of care.
Read the full article
Safety Spotlight: Maternal Deaths in the first trimester from Venous Thromboembolism (VTE)
MNSI has undertaken investigations of maternal deaths in the first trimester from venous thromboembolism (VTE)
Read the full article
Safety Spotlight: Changes to the MNSI investigation report template
On 1st April 2024, six months after the transition to being hosted by the CQC, MNSI changed their investigation reports and process.
Read the full article
Safety Spotlight: Incomplete observations generating incorrect EWS
MNSI has investigated a number of patient safety events where an incomplete set of observations generated an early warning score (EWS) via an electronic patient record (EPR) system.
Read the full article